A Nurse is Caring for a Client Recieving Continuous Bladder Irrigation Following
PURPOSE
To prevent blood clot formation, allow free flow of urine and maintain IDC patency, by continuously irrigating the bladder with Normal Saline
EXPECTED OUTCOMES
- The urinary catheter remains patent and urine is able to drain freely via the indwelling catheter (IDC)
- The patients comfort is maintained
- Clot formation within the bladder or IDC is prevented or minimised
- The patient's risk of Urinary Tract Infection is minimised, through use of aseptic technique when connecting bladder irrigation to IDC
EQUIPMENT FOR WARD BASED CONTINUOUS BLADDER IRRIGATION (CBI)
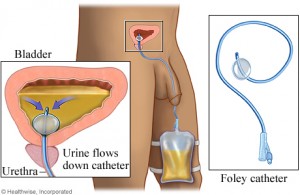
- 3way catheter
- 0.9% sodium Chloride irrigation bags as per facility policy
- Continuous bladder irrigation set and closed urinary drainage bag with anti-reflux valve.
- Alcohol wipes
- Non sterile gloves
- Personal protective equipment (PPE)
- Underpad (bluey)
- IV pole
1. Explain procedure to the patient and ensure patient privacy
2. Position the patient for easy access to the catheter whilst maintaining patient comfort
3. Ensure that the patient has a three-way urinary catheter.
4. Hang irrigation flasks on IV pole and prime irrigation set maintaining asepsis of irrigation set.
Note: Only one of the irrigation flask clamps should be open when priming the irrigation set otherwise the fluid can run from one flask to another. After priming the irrigation set ensure that all clamps on the irrigation set are closed
5. Don goggles and impervious gown , place underpad underneath catheter connection
6. Attend hand wash and don non-sterile gloves
7. Swab IDC irrigation and catheter ports with alcohol swabs and allow to dry
8. Open the irrigation lumen of the catheter
9. Connect the irrigation set to the irrigation lumen of the catheter, maintaining clean procedure
10. Ensure urine is draining freely before commencing continuous irrigation.
11. Unclamp the irrigation flask that was used to prime the irrigation set and set the rate of administration by adjusting the roller clamp.
Note: The aim of the bladder irrigation is to keep the urine rose' coloured and free from clots. The rate is determined and varied as required, not run at a set rate.
ONGOING MANAGEMENT
- Continue irrigation as necessary depending on the degree of haematuria (ensure adequate supply of irrigant nearby)
- After each flask is complete, empty urine drainage bag. Record urine output on the fluid balance chart, prior to commencement of the next irrigation flask
- Regular catheter care is required in order to minimise the risk of catheter related urinary tract infection
- Catheter care provided should be documented in the progress notes and nursing care plan including patient comfort, urine colour/degree of haematuria and urine output. Also presence of clots if any and if manual bladder washout was necessary
CLICK HERE for more resources on Fundamentals of Nursing
CLICK HERE for more resources on Laboratory & Diagnostic Test
- 1. Drainage out is less than irrigation infused
- Stop the irrigation. Recalculate I & O
- Ensure that tubing is not kinked or looped below bladder level
- Palpate bladder for distention. Use bladder scanner if available, to facilitate genitourinary assessment as per your unit's routine.
- If obstruction is suspected, gentle manual irrigation may be required as per physician's orders. Cleanse the
catheter opening well with chlorhexidine. Use nothing smaller than a 60cc syringe and sterile saline. Use slow,
even pressure to avoid damaging the bladder wall. Do not force if resistance met. Allow irrigation to flow
back freely - Notify physician if previous measures unsuccessful.
- Increase rate of irrigation infusion as per physician's orders.
- Irrigation of catheter as outlined in #1 to aid in clot removal may be indicated.
- If large amount blood or clots persists, notify physician
- Palpate bladder to determine presence of distention
- Check drainage tubing for kinks
- Observe drainage for adequate amount, presence of clots that might be blocking drainage tube. Evaluate I & O
- Avoid cold irrigation solution as it may cause bladder spasm.
- Assess if patient is orientated to time, place person
- Notify physician of patient's change in LOC
- Have relevant information ready to share with physician i.e. amount of opioids received, amount of CBI received,true urine output, time of onset of alteration in orientation, NA level; in TURP syndrome an overload of fluid through the prostatic sinuses can lead to dilutional hyponatremia, confusion and hypertension
- Assess for bladder spasms
- Refer to #1 – assessing for obstruction
- Consider administering antispasmatic i.e. Buscopan
2. Increased bloody drainage or presence of clots.
3. Patient complains of pain: (Complete pain assessment using the 0-10 or visual analogue scale)
4. The patient is confused/agitated
5. Solution Leaks around the foley catheter
Documentation:
Documentation includes:
- Patient's comfort/pain level (how procedure is being tolerated)
- Colour and type of drainage, presence of clots/fragments
- Intake and output
- Interventions required manual irrigation, use of bladder scanner
- Health teaching done with patient and family
- Patient concerns/adverse reactions (i.e. continued bladder spasms, decreased total urine output), the nursing actions taken and patient outcomes
CLICK HERE for more resources on Fundamentals of Nursing
CLICK HERE for more resources on Laboratory & Diagnostic Test
References:
Black et al (2001) Medical-Surgical Nursing, 6th edition, Toronto: W.B.Saunders
Perry, A. & Potter, P. (2002) Clinical Nursing Skills and Techniques 5th edition, St. Louis: Mosby
ACI UROLOGY NETWORK – Nursing Guidelines for bladder irrigation
Source: https://thenurseszone.com/continuous-bladder-irrigation-cbi/
{kind=link}
Post a Comment for "A Nurse is Caring for a Client Recieving Continuous Bladder Irrigation Following"